CT Scan for Renal Vascular Disease: Imaging Protocol Guide
CT Scan for Renal Vascular Disease: Imaging Protocol Guide

This article is part of our series of reference guides aimed at supporting computed tomography (CT) technologists in improving their clinical routines, enhancing the quality of the images they acquire, and delivering quality patient care. This guide focuses on renal CT scan imaging, addressing kidney anatomy, physiology, and CT scan protocols for imaging renal vascular disease.
A Quick Review of Kidney Anatomy and Physiology
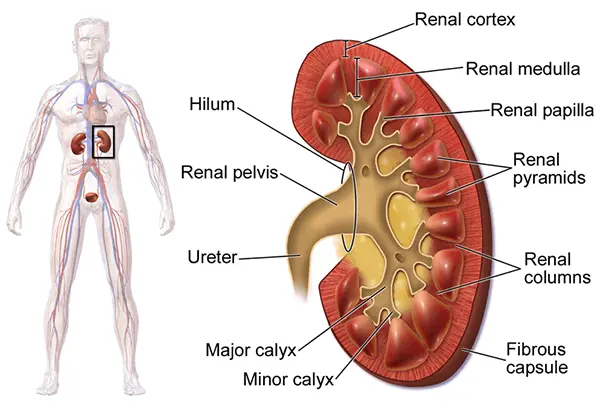
Located in the perirenal space, the kidneys are bean-shaped paired organs which lie parallel with the psoas muscles on each side of the lumbar spine. They measure about 9-13 cm in length with the lower pole of each kidney slightly anterior and lateral to the upper pole.1 The right kidney lies lower than the left kidney since the liver is in the right upper quadrant.
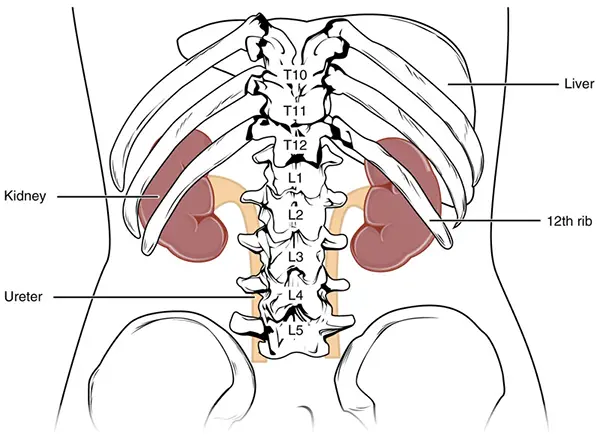
Source: https://commons.wikimedia.org/
A recessed fissure in the middle of the kidney, known as the renal hilum, allows the renal vessels, nerves, and collecting system to pass into the renal sinus. The outer renal cortex and the inner medullary space containing several renal pyramids make up the renal parenchyma.
The intrarenal collecting system consists of the calyces, infundibula, and renal pelvis. Urine flows from the calyx to the renal pelvis through the infundibula. The ureters move the urine by peristaltic contractions from the renal pelvis to the urinary bladder.
Source: https://commons.wikimedia.org/
CT Scan Protocols for Imaging Renal Vascular Disease
A procedure known as CT-KUB is a low-radiation dose CT which does not require intravenous or oral contrast and is the study of choice for locating stones (urolithiasis) in the kidneys, ureters, or bladder. However, its diagnostic performance for pathologies other than calculi is limited due to its lack of contrast and noise.
The protocol for performing a CT scan for renal masses is as follows: the patient is scanned following injection of 100-120 ml of contrast at a 3-5 ml/sec injection rate during the nephrogenic phase (complete enhancement of the renal parenchyma). This phase occurs about 90-120 seconds post-injection. The overall sensitivity of CT in the detection of renal masses is about 96%.
Obtain a few non-contrast scans (5mm) prior to injecting contrast. The key to an accurate evaluation of a renal mass is imaging in several different phases to look at the enhancement pattern and lesion borders.
- Remember to check for allergies prior to injecting contrast media.
- Additional laboratory testing, such as serum creatinine or eGFR, can be used to determine kidney function and ensure that the use of contrast dyes is safe.
- Verify that the patient has not had any recent diagnostic imaging studies involving contrast media, especially barium, which can cause artifacts and obscure the renal anatomy.
- Ensure that the patient is lying as flat as possible in the supine position.
- Start the scan above the left kidney (which is usually the higher kidney because the liver pushes the right kidney lower) and continue below the right kidney.
- Slice thickness is 2-5 mm with a 2-3 mm reconstruction interval.
- Most units are programmed at 120kVp for abdominal scans.
Artifacts
- Motion
- Metal or star artifacts
- Beam hardening (the result of attenuation of the beam as it passes through the patient)
- Partial volume effect (the effect of averaging data)
- Ring artifact – the result of a single detector going out of calibration

Case courtesy of Dr Omar Giyab, Radiopaedia.org. From the case rID: 22694
Protocol for Renal CT Angiography Scan
Multidetector CT angiography (CTA) has significantly improved image resolution and reduced the contrast dose for evaluation of the renal arteries with a one breath-hold. To ensure that there is optimal opacification of the artery, a bolus tracking method should be used. In addition to evaluating the abdominal aorta and renal arteries, CTA can assess other visceral arteries, renal size, cortical thickness, and detection of renal parenchymal abnormalities in the same study. CT angiography, when used for detection of renal artery stenosis, has high sensitivity (88% to 96%) and specificity (83% to 99%) rates.3 However, CTA requires the use of iodinated contrast media, which may be contraindicated in many patients with renal artery stenosis because of significantly impaired renal function.
Pathologies in Renal CT Scan
- Renal artery stenosis (RAS)
- Renal artery thrombosis
- Renal artery aneurysm (RAA)
- Renal vein thrombosis
- Atheroembolic renal disease
Renal artery stenosis (RAS) is the narrowing of one or both renal arteries which supply blood to the kidneys and help the body control blood pressure. Renovascular hypertension (RVHT) denotes nonessential hypertension where a causal relationship exists between anatomically evident arterial occlusive disease and elevated blood pressure. RAS is a major cause of RVHT and accounts for 1-10% of the 50 million cases of hypertension in the United States.
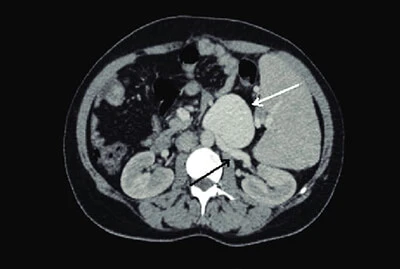
Computed angiography showing a large-sized renal vein aneurysm (white arrow) arising from the left renal vein (black arrow)
Source: https://www.researchgate.net/
A buildup of fatty deposits called plaque is the most common cause of renal artery stenosis. It can happen in either or both renal arteries and is often called “hardening of the arteries,” or atherosclerosis. The buildup can narrow the artery, reducing blood flow to the kidneys.4 Renal artery stenosis can also be caused by fibromuscular dysplasia—a condition in which some of the cells that line the renal arteries grow or do not develop correctly, which can cause the arteries to narrow.
- Sudden onset of flank (between the ribs and the upper border of the hip bone) pain and tenderness
- Fever
- Blood in the urine
- Nausea and/or vomiting
- Sudden decrease in kidney function
- Hypertension
Renal artery aneurysms, a bulging, weakened area in the wall of an artery to the kidney, are generally asymptomatic and may cause hypertension in up to ninety percent of people. Dissecting aneurysms, which are caused by a tear in the inner layer of the artery wall, may cause flank pain and blood in the urine.
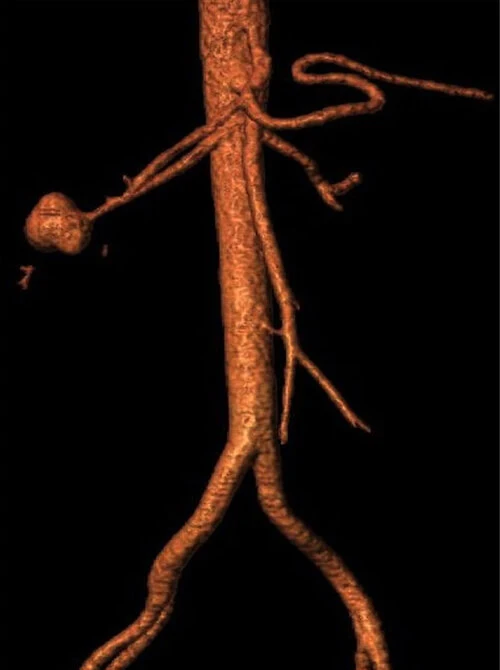
Three-dimensional reconstruction of a type III right renal artery aneurysm
Source: https://openheart.bmj.com/
When a clot forms in the renal vein, it is known as a renal vein thrombosis. This can be chronic or acute, which causes persistent severe flank pain, often spasmodic, and soreness in the area over the kidney. It can cause a decrease in the kidney function and is generally treated medically with anticoagulants.
And finally, atheroembolic renal disease occurs when a piece of plaque breaks off from the aorta and/or other large arteries and travels through the bloodstream. These pieces of plaque block small arteries such as the renal arteries. Atheroembolic renal disease is becoming a common cause of renal insufficiency (poor kidney function) in the elderly.
Treatment in Renal CT Scan
Treatment of a renal artery aneurysm depends on factors such as size and location of the aneurysm and whether symptoms are present. Certain types of small (less than two centimeters, or about three-quarters of an inch) aneurysms may not be treated but may be observed for growth or development of other complications. Many types of aneurysms may be treated surgically, such as aneurysms greater than two centimeters or three-quarters of an inch, dissecting aneurysms, aneurysms causing kidney ischemia or lack of blood flow to the kidney tissue, hypertension, aneurysms that are increasing in size, and aneurysms causing symptoms. Because of the increased risk for rupture (bursting), a renal artery aneurysm in a pregnant woman or a woman of child-bearing age will generally be treated surgically.
Renal artery stenosis is generally treated with renal angioplasty with stenting or renal bypass surgery. Renal masses can be treated with ablation or partial or radical nephrectomy depending on the size and type of the tumor.
Conclusion
CT plays an important role in the evaluation and management of primary renovascular disease and the secondary manifestations of such disease. CT angiography (CTA) with multiplanar reconstruction and three-dimensional display is valuable in studying patients with vascular processes involving the proximal renal vessels.
CT Advanced (8 CE credits) covers anatomy, head procedures, spine procedures, musculoskeletal procedures, chest and neck procedures, abdomen and pelvis procedures, and biopsies, drainages, and aspirations. Take the course risk-free with our 30-day refund policy and renew your ARRT® certification today.
Bibliography
- Lin, E., Coy, D. and Kanne, J., 2015. Body CT The Essentials. New York, N.Y: McGraw-Hill Education.
- Dunnick NR, Sandler; CM, Newhouse JH. Textbook of Uroradiology, 5th ed. Philadelphia, PA. Lippincott Williams & Wilkins;2013
- https://radiologykey.com/
- https://emedicine.medscape.com/
- Stanfordhealthcare.org. 2021. Renal Vascular Disease. [online] Available at: https://stanfordhealthcare.org/
- Lumsden AB, Salam TA, Walton KG. Renal artery aneurysm: a report of 28 cases. Cardiovasc Surg 1996; 4:185-189.
- Sultan S, Basuoniy Alawy M, Flaherty R, et al Endovascular management of renal artery aneurysms using the multilayer flow modulator Open Heart 2016;3: e000320. doi: 10.1136/openhrt-2015-000320
Suggested Readings
- https://radiologykey.com/
- https://radiopaedia.org/
- https://www.mayoclinic.org/
- https://www.uptodate.com/
- https://emedicine.medscape.com/
- https://stanfordhealthcare.org/
RELATED ARTICLES